








How you count beans matters. How you count coronavirus cases matters more.
The state of Oklahoma will be shifting some of the reporting procedures on its COVID-19 dashboard beginning Tuesday, health leaders announced at a media gaggle this morning.
“With this new system, we are actually going to be able to do more than we could before,” said Dr. Lance Frye, state commissioner of health.
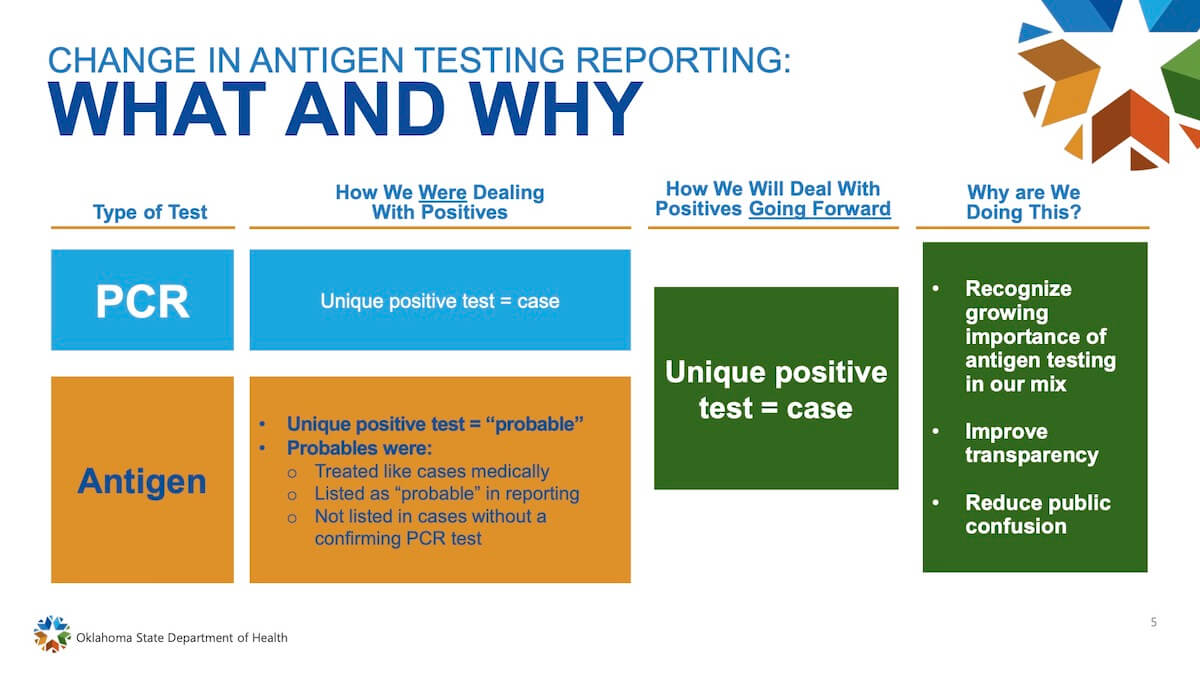
The shift focuses on a few things, chiefly the growing percentage of overall tests that are antigen tests, positive results of which have previously been considered “probable” cases and reported as a different pool of numbers.
Moving forward, positive antigen tests will be counted as “cases” on the state’s COVID-19 dashboard. To receive those results more efficiently from a variety of laboratories, the state is also preparing to put its antiquated PHIDDO reporting program to sleep (for COVID-19 only) and has been working with Google to create a new, more automated program to receive and report data.
“Right now we have the two programs running in parallel to make sure we don’t lose any data, and we are going to keep doing that until we have all the labs reporting (on the new system),” Frye said. “Our system was pretty old and was never built for a pandemic with the number of labs and [reports] that are coming in.”
One impetus for now considering positive antigen tests as “cases” stems from federal plans to distribute more antigen testing machines to long-term care facilities and schools by the end of the year.
“So we know those numbers are going to go up,” Frye said. “We are going to draw a line in the sand next week on Tuesday and start counting all of those as positives instead of probables.”
Frye said a small number of individuals considered to be an “epi-link” — which means someone who has not been tested but who is ill and lives with or has been linked to someone who has tested positive — will also be considered as cases moving forward.
So far, the state has seen about 5,000 antigen positives — previously considered “probables” — but Frye said those past antigen positives would not be retroactively considered as cases.
State epidemiologist Jared Taylor said the COVID-19 dashboard changes are “all about terminology” to comply with the federal Centers for Disease Control, which had previously considered antigen tests less reliable than PCR testing.
“CDC has this categorization of confirmed, probable and suspect. And we’ve always adhered to that categorization of confirmed, probable and suspect when reporting to the CDC. So those numbers are out there. (…) CDC ultimately had some revisions in the last few weeks of how they handled antigen tests.”
John Budd, Oklahoma’s chief operating officer, said any long-term care facility or school district that receives an antigen testing machine will be required to provide daily reporting updates to the state.
“The PHIDDO system has let us down multiple times, and you have gotten your data later than you wanted,” Budd told more than a dozen reporters at the State Capitol. “So if we tried to do the schools and the nursing homes with the PHIDDO system, it would be a catastrophe.”
Frye and Taylor said the new dashboard will also be better able to report the results of a new rapid COVID-19 test expected to hit the market this year.
“This is not the end of the new test. There are going to be multiple advances in testing and multiple different types of tests coming out, so we just want to make sure we are capturing all of those,” Frye said. “I really don’t know many details on those except it is going to be a rapid, self-collected test.”
Of numerators and denominators
Oklahoma will also change how it calculates a “percent positive” rate, moving it in line with the Johns Hopkins calculation.
“Currently, it is a real simple proportion of number of positive results divided by the total results,” Taylor said. “The Johns Hopkins methodology accounts for those individuals who get sampled multiple times as a positive.”
Frye said that will eliminate “repeat positives” from the state’s reporting.
“Everything we are doing right now is to make our data the best it can. We are trying to clean it up,” Frye said. “With this new system, we are going to be able to look at it more closely.”
Frye said states around the country are all making a variety of decisions about how to report coronavirus data.
“It’s the Wild West,” he said. “When you look around the nation, it’s all over the place as to what people do (for reporting).”
Taylor agreed.
“You can’t be conforming with everyone because everyone does it differently. So there have already been apparent discrepancies,” Taylor said. “We had landed upon the easiest calculation to do (…) at a time when we were struggling with data capacity. But we knew we couldn’t double count cases. You never want to double count cases. We’d had that all along, but now we’ve got a system that enables us to do this.”
“You’ve got to change at some point.”
Cases ‘will go up’ on COVID-19 dashboard
While the change in the calculation of percent positives will slightly decrease that statistic, the consideration of antigen tests as positives should increase the state’s overall caseload.
“It will go up. To start off with, I don’t think that number is going to be significant,” Frye said. “But that’s why we need to do it now because in the future as those tests get deployed, we are going to see it go up.”
Taylor said rural counties are currently relying more on antigen tests.
“In those, you’ll see a little bit more of a change,” he said. “When you get into the metro areas, you’re probably not going to see much of a change at all.”
Dr. George Monks, president of the Oklahoma State Medical Association, released a statement shortly after Friday’s briefing praising state leaders.
“The best medicine relies on the best data. As physicians, we are grateful to the Oklahoma State Department of Health for improving the quality and accuracy of their reporting through a system upgrade through their new partnership with Google,” Monks said. “Furthermore, we are pleased to hear that they will soon begin, including rapid antigen test results in their daily reports. As these tests become more widely-used throughout Oklahoma, the information they provide could help more quickly identify those who have been exposed to coronavirus. These results will be instrumental in helping slow the spread throughout densely-populated areas such as schools, colleges and nursing homes, where quick identification of the disease can save countless lives. In addition, antigen tests can give contact tracers a much-needed boost in their efforts to identify people who have been exposed to those with COVID-19 and notify others of potential risks.”
Vaccine development, contact tracing discussed
State health leaders also briefly discussed contact tracing and potential COVID-19 vaccines.
“It’s a means to try to control the spread of the disease by contacting those people,” Frye said of contact tracing. “The fundamental purpose is to identify potential contacts of someone who tested positive. So you would like to contact those people and advise them — you want to find out if that contact was what we would consider of any significance. And then if it was, give those people advice on how to manage that situation.”
But Taylor noted the current limitations of using contact tracing data to determine where transmission of the virus is occuring.
“The data is overwhelming while also being incomplete and largely unparsable at this point. What we could do is we could have a characterization of where individuals reported having contacted people. But that’s not indicative of transmission, per se,” Taylor said. “All of this stuff that we are talking about and more is going to facilitate our efforts. That is critical. But even once we do that, it’s going to be really important to acknowledge the limitations of that.”
On the topic of vaccine development, deputy commissioner of health Keith Reed said the CDC has told states to be prepared for a potential vaccine deployment in October or November. He said Oklahoma would prioritize certain populations once a vaccine is available, such as health care workers, first responders and seniors with a higher risk of morbidity.
Reed said drive-thru dispersement of a vaccine could be an option.
“I’m not worried about our ability to get it out,” he said. “I’m more worried about our rapid supply chain coming in to get it out.”
Frye said he would have no concerns about getting a COVID-19 vaccine.
“They vaccinated me against everything in the military,” Frye said. “I don’t have any concerns about that at all.”
(Update: This story was updated at 11:30 a.m. Friday, Sept. 4, to include comment from Dr. George Monks.)












{kind=link}